Fallen Arches What You Need
Overview
Fallen arches, the medical term for flat feet, are simply feet that do not arch in the middle. Such feet lay flat with the whole of the sole on the ground. All children are born with flat feet, but as they grow the feet normally develop an arch so that by the age of ten almost all children have arched feet. Occasionally a child will not develop properly arched feet. This may be due to a bone malformation present at birth, or abnormalities in ligaments within the feet or legs that cause the child's weight to be unevenly distributed.
Causes
The arches of most individuals are fully developed by the age of 12 to 13. While some people are born with flat arches, for others, the arches fall over time. The tibial tendon, which runs along the inside of the ankle from above the ankle to the arch, can weaken with age and with heavy activity. The posterior tendon, main support structure for the arch, can become inflamed (tendonitis) or even tear if overloaded. For women, wearing high heels can affect the Achilles tendon and alter the structure and function of the ankle. The posterior tibial tendon may compensate for this stress and break down, causing the arches to fall. Obesity is another contributing factor, as well as a serious injury to the ankle or foot, arthritis and bad circulation such as occurs with diabetes.
Symptoms
Most people do not exhibit any symptoms of flat feet, but if the condition is due to an underlying problem, symptoms can include foot pain, mainly in the arch or heel areas, difficulty standing on tiptoes, swelling that occurs on the inside of the ankle, pain in the calf, knee, hip, or lower leg area, both feet lie flat on the ground with no gap, Shoes may not fit properly, heel may tilt away from the midline of the body more than usual, absence of foot arch when standing. If you are experiencing these symptoms and have flat feet, you should consider seeing your doctor or a podiatrist immediately for an examination.
Diagnosis
Determining whether you have fallen arches may be as easy as looking at the shape of the middle bottom of your foot. Is there any kind of arch there? If you cannot find any kind of arch, you may have a flat foot. There are, however, other ways to decide in case you're still not sure. Another way to figure out if you have flat feet is to look at a few pairs of your shoes. Where do you see the most wear on the heels? If you notice significant wear in the heel and the ball of the foot extending to the big toe, this means you are overpronating. Overpronators roll their feet too far inward and commonly have fallen arches. To figure out if you have flat feet, you can also do an easy test. Get the bottoms of your feet wet and then step on to a piece of paper carefully. Step off the paper and take a look at the print your foot made. If your print looks like the entire bottom of a foot, your feet are flat. People with an arch will be missing part of the foot on their print since the arch is elevated off of the paper. Regular visits to your podiatrist are highly recommended.
fallen arches insoles
Non Surgical Treatment
Have you found yourself in the store looking at all the different foot care products? There is everything from massaging gel insoles to foam arch supports and heel cushions. If your arches fall the same amount on each side, you might be able to use an insert off the shelf. If they fall differently, then a generic insert will not fix the imbalance. If you have a high arch, a generic insert will likely not be high enough for full correction. Good custom orthotics provide a number of advantages over the generic inserts that you find in the store. Custom orthotics can take into account your body weight and degree of flexibility in your foot, not someone else?s. They also account for the anatomical differences in your feet. The corrected height of one arch is often higher in one foot than the other. A G-Laser foot analysis can provide you with this information.
Surgical Treatment

This is rare and usually only offered if patients have significant abnormalities in their bones or muscles. Treatments include joint fusion, reshaping the bones in the foot, and occasionally moving around tendons in the foot to help balance out the stresses (called tendon transfer). Flat feet and fallen arches are common conditions that are in most cases asymptomatic. However, in patients who do have symptoms, treatments are available that can help reduce pain and promote efficient movement. Orthotic devices are well recognised as an excellent treatment and podiatrists can offer these different treatment modalities as individualised treatments for patients.
After Care
Patients may go home the day of surgery or they may require an overnight hospital stay. The leg will be placed in a splint or cast and should be kept elevated for the first two weeks. At that point, sutures are removed. A new cast or a removable boot is then placed. It is important that patients do not put any weight on the corrected foot for six to eight weeks following the operation. Patients may begin bearing weight at eight weeks and usually progress to full weightbearing by 10 to 12 weeks. For some patients, weightbearing requires additional time. After 12 weeks, patients commonly can transition to wearing a shoe. Inserts and ankle braces are often used. Physical therapy may be recommended. There are complications that relate to surgery in general. These include the risks associated with anesthesia, infection, damage to nerves and blood vessels, and bleeding or blood clots. Complications following flatfoot surgery may include wound breakdown or nonunion (incomplete healing of the bones). These complications often can be prevented with proper wound care and rehabilitation. Occasionally, patients may notice some discomfort due to prominent hardware. Removal of hardware can be done at a later time if this is an issue. The overall complication rates for flatfoot surgery are low.
Fallen arches, the medical term for flat feet, are simply feet that do not arch in the middle. Such feet lay flat with the whole of the sole on the ground. All children are born with flat feet, but as they grow the feet normally develop an arch so that by the age of ten almost all children have arched feet. Occasionally a child will not develop properly arched feet. This may be due to a bone malformation present at birth, or abnormalities in ligaments within the feet or legs that cause the child's weight to be unevenly distributed.
Causes
The arches of most individuals are fully developed by the age of 12 to 13. While some people are born with flat arches, for others, the arches fall over time. The tibial tendon, which runs along the inside of the ankle from above the ankle to the arch, can weaken with age and with heavy activity. The posterior tendon, main support structure for the arch, can become inflamed (tendonitis) or even tear if overloaded. For women, wearing high heels can affect the Achilles tendon and alter the structure and function of the ankle. The posterior tibial tendon may compensate for this stress and break down, causing the arches to fall. Obesity is another contributing factor, as well as a serious injury to the ankle or foot, arthritis and bad circulation such as occurs with diabetes.
Symptoms
Most people do not exhibit any symptoms of flat feet, but if the condition is due to an underlying problem, symptoms can include foot pain, mainly in the arch or heel areas, difficulty standing on tiptoes, swelling that occurs on the inside of the ankle, pain in the calf, knee, hip, or lower leg area, both feet lie flat on the ground with no gap, Shoes may not fit properly, heel may tilt away from the midline of the body more than usual, absence of foot arch when standing. If you are experiencing these symptoms and have flat feet, you should consider seeing your doctor or a podiatrist immediately for an examination.
Diagnosis
Determining whether you have fallen arches may be as easy as looking at the shape of the middle bottom of your foot. Is there any kind of arch there? If you cannot find any kind of arch, you may have a flat foot. There are, however, other ways to decide in case you're still not sure. Another way to figure out if you have flat feet is to look at a few pairs of your shoes. Where do you see the most wear on the heels? If you notice significant wear in the heel and the ball of the foot extending to the big toe, this means you are overpronating. Overpronators roll their feet too far inward and commonly have fallen arches. To figure out if you have flat feet, you can also do an easy test. Get the bottoms of your feet wet and then step on to a piece of paper carefully. Step off the paper and take a look at the print your foot made. If your print looks like the entire bottom of a foot, your feet are flat. People with an arch will be missing part of the foot on their print since the arch is elevated off of the paper. Regular visits to your podiatrist are highly recommended.
fallen arches insoles
Non Surgical Treatment
Have you found yourself in the store looking at all the different foot care products? There is everything from massaging gel insoles to foam arch supports and heel cushions. If your arches fall the same amount on each side, you might be able to use an insert off the shelf. If they fall differently, then a generic insert will not fix the imbalance. If you have a high arch, a generic insert will likely not be high enough for full correction. Good custom orthotics provide a number of advantages over the generic inserts that you find in the store. Custom orthotics can take into account your body weight and degree of flexibility in your foot, not someone else?s. They also account for the anatomical differences in your feet. The corrected height of one arch is often higher in one foot than the other. A G-Laser foot analysis can provide you with this information.
Surgical Treatment
This is rare and usually only offered if patients have significant abnormalities in their bones or muscles. Treatments include joint fusion, reshaping the bones in the foot, and occasionally moving around tendons in the foot to help balance out the stresses (called tendon transfer). Flat feet and fallen arches are common conditions that are in most cases asymptomatic. However, in patients who do have symptoms, treatments are available that can help reduce pain and promote efficient movement. Orthotic devices are well recognised as an excellent treatment and podiatrists can offer these different treatment modalities as individualised treatments for patients.
After Care
Patients may go home the day of surgery or they may require an overnight hospital stay. The leg will be placed in a splint or cast and should be kept elevated for the first two weeks. At that point, sutures are removed. A new cast or a removable boot is then placed. It is important that patients do not put any weight on the corrected foot for six to eight weeks following the operation. Patients may begin bearing weight at eight weeks and usually progress to full weightbearing by 10 to 12 weeks. For some patients, weightbearing requires additional time. After 12 weeks, patients commonly can transition to wearing a shoe. Inserts and ankle braces are often used. Physical therapy may be recommended. There are complications that relate to surgery in general. These include the risks associated with anesthesia, infection, damage to nerves and blood vessels, and bleeding or blood clots. Complications following flatfoot surgery may include wound breakdown or nonunion (incomplete healing of the bones). These complications often can be prevented with proper wound care and rehabilitation. Occasionally, patients may notice some discomfort due to prominent hardware. Removal of hardware can be done at a later time if this is an issue. The overall complication rates for flatfoot surgery are low.
Leg Length Discrepancy Barefoot Running
Overview
Leg length discrepancy is the difference in lengths of an individual?s legs. This difference may be anatomical or may be due to scoliosis, trauma/injury, arthritis, overpronation (collapse) of one foot, bowing of one leg or unequal bowing, surgery (hip or knee replacement), pelvic tilting or ageing. The difference can also be functional caused by differing forces of the soft tissues, such as weakness in muscle tissue on one side, or a weakness/tightness in joint tissue. A difference in leg lengths also results when running on indoor banked tracks, beaches and banked streets and side walks (for drainage). Many people have a measurable difference in their leg lengths which is compensated for by their bodies. As we age this compensation does not work as well. An x-ray and physical measurements will define the discrepancy and the adjustment needed.
Causes
Sometimes the cause of LLD is unknown, yet the pattern or combination of conditions is consistent with a certain abnormality. Examples include underdevelopment of the inner or outer side of the leg (hemimelias) or (partial) inhibition of growth of one side of the body of unknown cause (hemihypertrophy). These conditions are present at birth, but the limb length difference may be too small to be detected. As the child grows, the LLD increases and becomes more noticeable. In hemimelia, one of the two bones between the knee and the ankle (tibia or fibula) is abnormally short. There also may be associated foot or knee abnormalities. Hemihypertrophy or hemiatrophy are rare conditions in which there is a difference in length of both the arm and leg on only one side of the body. There may also be a difference between the two sides of the face. Sometimes no cause can be found. This type of limb length is called idiopathic. While there is a cause, it cannot be determined using currect diagnostic methods.
Symptoms
Back pain along with pain in the foot, knee, leg and hip on one side of the body are the main complaints. There may also be limping or head bop down on the short side or uneven arm swinging. The knee bend, hip or shoulder may be down on one side, and there may be uneven wear to the soles of shoes (usually more on the longer side).
Diagnosis
The most accurate method to identify leg (limb) length inequality (discrepancy) is through radiography. It?s also the best way to differentiate an anatomical from a functional limb length inequality. Radiography, A single exposure of the standing subject, imaging the entire lower extremity. Limitations are an inherent inaccuracy in patients with hip or knee flexion contracture and the technique is subject to a magnification error. Computed Tomography (CT-scan), It has no greater accuracy compared to the standard radiography. The increased cost for CT-scan may not be justified, unless a contracture of the knee or hip has been identified or radiation exposure must be minimized. However, radiography has to be performed by a specialist, takes more time and is costly. It should only be used when accuracy is critical. Therefore two general clinical methods were developed for assessing LLI. Direct methods involve measuring limb length with a tape measure between 2 defined points, in stand. Two common points are the anterior iliac spine and the medial malleolus or the anterior inferior iliac spine and lateral malleolus. Be careful, however, because there is a great deal of criticism and debate surrounds the accuracy of tape measure methods. If you choose for this method, keep following topics and possible errors in mind. Always use the mean of at least 2 or 3 measures. If possible, compare measures between 2 or more clinicians. Iliac asymmetries may mask or accentuate a limb length inequality. Unilateral deviations in the long axis of the lower limb (eg. Genu varum,?) may mask or accentuate a limb length inequality. Asymmetrical position of the umbilicus. Joint contractures. Indirect methods. Palpation of bony landmarks, most commonly the iliac crests or anterior iliac spines, in stand. These methods consist in detecting if bony landmarks are at (horizontal) level or if limb length inequality is present. Palpation and visual estimation of the iliac crest (or SIAS) in combination with the use of blocks or book pages of known thickness under the shorter limb to adjust the level of the iliac crests (or SIAS) appears to be the best (most accurate and precise) clinical method to asses limb inequality. You should keep in mind that asymmetric pelvic rotations in planes other than the frontal plane may be associated with limb length inequality. A review of the literature suggest, therefore, that the greater trochanter major and as many pelvic landmarks should be palpated and compared (left trochanter with right trochanter) when the block correction method is used.
Non Surgical Treatment
Treatment of leg length inequality involves many different approaches, which vary among osteopaths, physiotherapist and chiropractor and whether the LLD is functional or structural. Thus is a combination of myofascial release (massage) & stretching of shortened muscles. Manipulation or mobilization of the spine, sacro-iliac joint (SIJ), hip, knee, foot. Orthotics, shoe lifts can be used to treat discrepancies from two to six cm (usually up to 1 cm can be inserted in the shoe. For larger leg length inequalities, the shoe must be built up. This needs to be done for every shoe worn, thus limiting the type of shoe that the patient can wear). Surgery (epiphysiodesis, epiphyseal stapling,bone resection).

what can i do to get taller?
Surgical Treatment
Bone growth restriction (epiphysiodesis) The objective of this surgical procedure is to slow down growth in the longer leg. During surgery, doctors alter the growth plate of the bone in the longer leg by inserting a small plate or staples. This slows down growth, allowing the shorter leg to catch up over time. Your child may spend a night in the hospital after this procedure or go home the same day. Doctors may place a knee brace on the leg for a few days. It typically takes 2 to 3 months for the leg to heal completely. An alternative approach involves lengthening the shorter bone. We are more likely to recommend this approach if your child is on the short side of the height spectrum.
Leg length discrepancy is the difference in lengths of an individual?s legs. This difference may be anatomical or may be due to scoliosis, trauma/injury, arthritis, overpronation (collapse) of one foot, bowing of one leg or unequal bowing, surgery (hip or knee replacement), pelvic tilting or ageing. The difference can also be functional caused by differing forces of the soft tissues, such as weakness in muscle tissue on one side, or a weakness/tightness in joint tissue. A difference in leg lengths also results when running on indoor banked tracks, beaches and banked streets and side walks (for drainage). Many people have a measurable difference in their leg lengths which is compensated for by their bodies. As we age this compensation does not work as well. An x-ray and physical measurements will define the discrepancy and the adjustment needed.
Causes
Sometimes the cause of LLD is unknown, yet the pattern or combination of conditions is consistent with a certain abnormality. Examples include underdevelopment of the inner or outer side of the leg (hemimelias) or (partial) inhibition of growth of one side of the body of unknown cause (hemihypertrophy). These conditions are present at birth, but the limb length difference may be too small to be detected. As the child grows, the LLD increases and becomes more noticeable. In hemimelia, one of the two bones between the knee and the ankle (tibia or fibula) is abnormally short. There also may be associated foot or knee abnormalities. Hemihypertrophy or hemiatrophy are rare conditions in which there is a difference in length of both the arm and leg on only one side of the body. There may also be a difference between the two sides of the face. Sometimes no cause can be found. This type of limb length is called idiopathic. While there is a cause, it cannot be determined using currect diagnostic methods.
Symptoms
Back pain along with pain in the foot, knee, leg and hip on one side of the body are the main complaints. There may also be limping or head bop down on the short side or uneven arm swinging. The knee bend, hip or shoulder may be down on one side, and there may be uneven wear to the soles of shoes (usually more on the longer side).
Diagnosis
The most accurate method to identify leg (limb) length inequality (discrepancy) is through radiography. It?s also the best way to differentiate an anatomical from a functional limb length inequality. Radiography, A single exposure of the standing subject, imaging the entire lower extremity. Limitations are an inherent inaccuracy in patients with hip or knee flexion contracture and the technique is subject to a magnification error. Computed Tomography (CT-scan), It has no greater accuracy compared to the standard radiography. The increased cost for CT-scan may not be justified, unless a contracture of the knee or hip has been identified or radiation exposure must be minimized. However, radiography has to be performed by a specialist, takes more time and is costly. It should only be used when accuracy is critical. Therefore two general clinical methods were developed for assessing LLI. Direct methods involve measuring limb length with a tape measure between 2 defined points, in stand. Two common points are the anterior iliac spine and the medial malleolus or the anterior inferior iliac spine and lateral malleolus. Be careful, however, because there is a great deal of criticism and debate surrounds the accuracy of tape measure methods. If you choose for this method, keep following topics and possible errors in mind. Always use the mean of at least 2 or 3 measures. If possible, compare measures between 2 or more clinicians. Iliac asymmetries may mask or accentuate a limb length inequality. Unilateral deviations in the long axis of the lower limb (eg. Genu varum,?) may mask or accentuate a limb length inequality. Asymmetrical position of the umbilicus. Joint contractures. Indirect methods. Palpation of bony landmarks, most commonly the iliac crests or anterior iliac spines, in stand. These methods consist in detecting if bony landmarks are at (horizontal) level or if limb length inequality is present. Palpation and visual estimation of the iliac crest (or SIAS) in combination with the use of blocks or book pages of known thickness under the shorter limb to adjust the level of the iliac crests (or SIAS) appears to be the best (most accurate and precise) clinical method to asses limb inequality. You should keep in mind that asymmetric pelvic rotations in planes other than the frontal plane may be associated with limb length inequality. A review of the literature suggest, therefore, that the greater trochanter major and as many pelvic landmarks should be palpated and compared (left trochanter with right trochanter) when the block correction method is used.
Non Surgical Treatment
Treatment of leg length inequality involves many different approaches, which vary among osteopaths, physiotherapist and chiropractor and whether the LLD is functional or structural. Thus is a combination of myofascial release (massage) & stretching of shortened muscles. Manipulation or mobilization of the spine, sacro-iliac joint (SIJ), hip, knee, foot. Orthotics, shoe lifts can be used to treat discrepancies from two to six cm (usually up to 1 cm can be inserted in the shoe. For larger leg length inequalities, the shoe must be built up. This needs to be done for every shoe worn, thus limiting the type of shoe that the patient can wear). Surgery (epiphysiodesis, epiphyseal stapling,bone resection).
what can i do to get taller?
Surgical Treatment
Bone growth restriction (epiphysiodesis) The objective of this surgical procedure is to slow down growth in the longer leg. During surgery, doctors alter the growth plate of the bone in the longer leg by inserting a small plate or staples. This slows down growth, allowing the shorter leg to catch up over time. Your child may spend a night in the hospital after this procedure or go home the same day. Doctors may place a knee brace on the leg for a few days. It typically takes 2 to 3 months for the leg to heal completely. An alternative approach involves lengthening the shorter bone. We are more likely to recommend this approach if your child is on the short side of the height spectrum.
Understanding Heel Discomfort
Overview
Heel pain is one of the most common conditions treated by podiatrists. It is often a message from the body that something is in need of medical attention. Pain that occurs right after an injury or early in an illness may play a protective role, often warning us about the damage we have suffered. The greatest incidence of heel pain is seen in middle-aged men and women. It is also seen in those who take part in regular sporting activities and those significantly overweight and on their feet a lot. Heel pain can also occur in children, usually between 8 and 13, as they become increasingly active in sporting activities.
Causes
Some of the many causes of heel pain can include abnormal walking style (gait), such as rolling the feet inwards. Obesity. Ill-fitting shoes. Standing, running or jumping on hard surfaces. Injury to the heel, such as stress fractures. Bursitis (inflammation of a bursa, bursae are small sacs that contain fluid to lubricate moving parts, such as joints and muscles). Neuroma (nerve enlargement). Certain disorders, including diabetes and arthritis.
Symptoms
Initially, this pain may only be present when first standing up after sleeping or sitting. As you walk around, the muscle and tendon loosen and the pain goes away. As this problem progresses, the pain can be present with all standing and walking. You may notice a knot or bump on the back of the heel. Swelling may develop. In some cases, pressure from the back of the shoe causes pain.
Diagnosis
In most cases, your GP or a podiatrist (a specialist in foot problems and foot care) should be able to diagnose the cause of your heel pain by asking about your symptoms and medical history, examining your heel and foot.
Non Surgical Treatment
Initially, treatment will consist of adding support to the foot, including better shoes and an over-the-counter arch supports and/or insoles; resting from the sport or activity that aggravates the problem; stretching the calf and arch muscles; taking anti-inflammatory; and using ice and massage to reduce inflammation. You can ice and message your muscles simultaneously by freezing a water bottle filled with water and using it to massage your foot by rolling it underneath your foot for five to 10 minutes at least two times per day. It is not unusual for symptoms of plantar fasciitis to persist for six to 12 months despite treatment.
Surgical Treatment
With the advancements in technology and treatments, if you do need to have surgery for the heel, it is very minimal incision that?s done. And the nice thing is your recovery period is short and you should be able to bear weight right after the surgery. This means you can get back to your weekly routine in just a few weeks. Recovery is a lot different than it used to be and a lot of it is because of doing a minimal incision and decreasing trauma to soft tissues, as well as even the bone. So if you need surgery, then your recovery period is pretty quick.
heel spur treatment natural remedies
Prevention

You can try to avoid the things that cause heel pain to start avoid becoming overweight, where your job allows, minimise the shock to your feet from constant pounding on hard surfaces, reduce the shocks on your heel by choosing footwear with some padding or shock-absorbing material in the heel, if you have high-arched feet or flat feet a moulded insole in your shoe may reduce the stresses on your feet, if you have an injury to your ankle or foot, make sure you exercise afterwards to get back as much movement as possible to reduce the stresses on your foot and your heel in particular, If you start to get heel pain, doing the above things may enable the natural healing process to get underway and the pain to improve.
Heel pain is one of the most common conditions treated by podiatrists. It is often a message from the body that something is in need of medical attention. Pain that occurs right after an injury or early in an illness may play a protective role, often warning us about the damage we have suffered. The greatest incidence of heel pain is seen in middle-aged men and women. It is also seen in those who take part in regular sporting activities and those significantly overweight and on their feet a lot. Heel pain can also occur in children, usually between 8 and 13, as they become increasingly active in sporting activities.
Causes
Some of the many causes of heel pain can include abnormal walking style (gait), such as rolling the feet inwards. Obesity. Ill-fitting shoes. Standing, running or jumping on hard surfaces. Injury to the heel, such as stress fractures. Bursitis (inflammation of a bursa, bursae are small sacs that contain fluid to lubricate moving parts, such as joints and muscles). Neuroma (nerve enlargement). Certain disorders, including diabetes and arthritis.
Symptoms
Initially, this pain may only be present when first standing up after sleeping or sitting. As you walk around, the muscle and tendon loosen and the pain goes away. As this problem progresses, the pain can be present with all standing and walking. You may notice a knot or bump on the back of the heel. Swelling may develop. In some cases, pressure from the back of the shoe causes pain.
Diagnosis
In most cases, your GP or a podiatrist (a specialist in foot problems and foot care) should be able to diagnose the cause of your heel pain by asking about your symptoms and medical history, examining your heel and foot.
Non Surgical Treatment
Initially, treatment will consist of adding support to the foot, including better shoes and an over-the-counter arch supports and/or insoles; resting from the sport or activity that aggravates the problem; stretching the calf and arch muscles; taking anti-inflammatory; and using ice and massage to reduce inflammation. You can ice and message your muscles simultaneously by freezing a water bottle filled with water and using it to massage your foot by rolling it underneath your foot for five to 10 minutes at least two times per day. It is not unusual for symptoms of plantar fasciitis to persist for six to 12 months despite treatment.
Surgical Treatment
With the advancements in technology and treatments, if you do need to have surgery for the heel, it is very minimal incision that?s done. And the nice thing is your recovery period is short and you should be able to bear weight right after the surgery. This means you can get back to your weekly routine in just a few weeks. Recovery is a lot different than it used to be and a lot of it is because of doing a minimal incision and decreasing trauma to soft tissues, as well as even the bone. So if you need surgery, then your recovery period is pretty quick.
heel spur treatment natural remedies
Prevention
You can try to avoid the things that cause heel pain to start avoid becoming overweight, where your job allows, minimise the shock to your feet from constant pounding on hard surfaces, reduce the shocks on your heel by choosing footwear with some padding or shock-absorbing material in the heel, if you have high-arched feet or flat feet a moulded insole in your shoe may reduce the stresses on your feet, if you have an injury to your ankle or foot, make sure you exercise afterwards to get back as much movement as possible to reduce the stresses on your foot and your heel in particular, If you start to get heel pain, doing the above things may enable the natural healing process to get underway and the pain to improve.
Mortons Neuroma Prevention
Overview
 A Morton's neuroma is a benign (noncancerous) swelling along a nerve in the foot that carries sensations from the toes. The reason the nerve starts to swell is unknown. But once swelling begins, the nearby bones and ligaments put pressure on the nerve, causing more irritation and inflammation. This produces burning pain, numbness, tingling and other abnormal sensations in the toes. A Morton's neuroma also is called an interdigital neuroma, intermetatarsal neuroma or a forefoot neuroma.
A Morton's neuroma is a benign (noncancerous) swelling along a nerve in the foot that carries sensations from the toes. The reason the nerve starts to swell is unknown. But once swelling begins, the nearby bones and ligaments put pressure on the nerve, causing more irritation and inflammation. This produces burning pain, numbness, tingling and other abnormal sensations in the toes. A Morton's neuroma also is called an interdigital neuroma, intermetatarsal neuroma or a forefoot neuroma.
Causes
The exact cause of Morton?s neuroma is not known, but the choice of footwear seems be a factor. Wearing high heels (shoes with heels over 2 inches) can put extra pressure on the balls of the feet. Wearing tight or pointed toed shoes may squeeze the toes together or otherwise constrict their movement. For that reason, women are about 8 to 10 times more likely to develop Morton?s neuroma compared with men. People who are born with flat feet, high arches, or an abnormal position of the toes are more prone to developing Morton?s neuroma. This may be due to instability around the toe joints. Certain conditions that develop over time, such as bunions or hammer toes, are also associated with Morton?s neuroma. Some sports that involve running, including tennis and other racquet sports, can also increase the chance of developing Morton?s neuroma due to trauma or injury to the foot.
Symptoms
Symptoms of interdigital neuroma typically manifest as a sharp, burning or tingling sensation in the forefoot. The pain radiates toward the lesser toes and is aggravated by shoe wear. The pain is relieved when the shoe is removed and the forefoot is massaged. Sometimes the symptoms involve specific toes.
Diagnosis
Patients with classic Morton?s neuroma symptoms will have pain with pressure at the base of the involved toes (either between the 2nd and 3rd toes, or between the 3rd and 4th toes). In addition, squeezing the front of the foot together can exacerbate symptoms. As well, they may have numbness on the sides of one toe and the adjacent toe, as this corresponds with the distribution of the involved nerve.
Non Surgical Treatment
Conservative treatment involves a reduction in the inflammation and removing the impingement factor. Reduction in inflammation is achieved via rest, elevation, ice, and massage with anti-inflammatory gels. Removing foot wear and and/r wearing broad type footwear would also help. Injection therapy is useful in reducing symptoms but not very successful in providing long term relief. The only time when it is most appropriate is when the cause of the space occupying object is not a neuroma but an inflamed bursa. Injection would help to relieve symptoms, and often cortisone is not even necessary.
Surgical Treatment
Surgery to excise the neuroma is usually performed under general anaesthetic in a day surgery facility. After surgery you will have to keep your foot dry for two weeks. Generally neuroma surgery allows for early weight bearing and protection in some type of post op shoe gear. Some neuromas may reoccur, but this is rare. Most studies on patient satisfaction after neuroma surgery show approximately 90% reduction of pain and about 85% of all patients rated the overall satisfaction with the results as excellent or good.
A Morton's neuroma is a benign (noncancerous) swelling along a nerve in the foot that carries sensations from the toes. The reason the nerve starts to swell is unknown. But once swelling begins, the nearby bones and ligaments put pressure on the nerve, causing more irritation and inflammation. This produces burning pain, numbness, tingling and other abnormal sensations in the toes. A Morton's neuroma also is called an interdigital neuroma, intermetatarsal neuroma or a forefoot neuroma.Causes
The exact cause of Morton?s neuroma is not known, but the choice of footwear seems be a factor. Wearing high heels (shoes with heels over 2 inches) can put extra pressure on the balls of the feet. Wearing tight or pointed toed shoes may squeeze the toes together or otherwise constrict their movement. For that reason, women are about 8 to 10 times more likely to develop Morton?s neuroma compared with men. People who are born with flat feet, high arches, or an abnormal position of the toes are more prone to developing Morton?s neuroma. This may be due to instability around the toe joints. Certain conditions that develop over time, such as bunions or hammer toes, are also associated with Morton?s neuroma. Some sports that involve running, including tennis and other racquet sports, can also increase the chance of developing Morton?s neuroma due to trauma or injury to the foot.
Symptoms
Symptoms of interdigital neuroma typically manifest as a sharp, burning or tingling sensation in the forefoot. The pain radiates toward the lesser toes and is aggravated by shoe wear. The pain is relieved when the shoe is removed and the forefoot is massaged. Sometimes the symptoms involve specific toes.
Diagnosis
Patients with classic Morton?s neuroma symptoms will have pain with pressure at the base of the involved toes (either between the 2nd and 3rd toes, or between the 3rd and 4th toes). In addition, squeezing the front of the foot together can exacerbate symptoms. As well, they may have numbness on the sides of one toe and the adjacent toe, as this corresponds with the distribution of the involved nerve.
Non Surgical Treatment
Conservative treatment involves a reduction in the inflammation and removing the impingement factor. Reduction in inflammation is achieved via rest, elevation, ice, and massage with anti-inflammatory gels. Removing foot wear and and/r wearing broad type footwear would also help. Injection therapy is useful in reducing symptoms but not very successful in providing long term relief. The only time when it is most appropriate is when the cause of the space occupying object is not a neuroma but an inflamed bursa. Injection would help to relieve symptoms, and often cortisone is not even necessary.
Surgical Treatment
Surgery to excise the neuroma is usually performed under general anaesthetic in a day surgery facility. After surgery you will have to keep your foot dry for two weeks. Generally neuroma surgery allows for early weight bearing and protection in some type of post op shoe gear. Some neuromas may reoccur, but this is rare. Most studies on patient satisfaction after neuroma surgery show approximately 90% reduction of pain and about 85% of all patients rated the overall satisfaction with the results as excellent or good.
Leg Length Discrepancy And Shoe Lifts
There are actually two different types of leg length discrepancies, congenital and acquired. Congenital means you are born with it. One leg is anatomically shorter than the other. As a result of developmental phases of aging, the human brain picks up on the gait pattern and recognizes some difference. Our bodies typically adapts by tilting one shoulder over to the "short" side. A difference of under a quarter inch is not blatantly irregular, doesn't need Shoe Lifts to compensate and typically does not have a serious effect over a lifetime.

Leg length inequality goes largely undiscovered on a daily basis, yet this problem is very easily solved, and can eradicate a number of incidents of back ache.
Treatment for leg length inequality usually involves Shoe Lifts. These are generally cost-effective, usually priced at under twenty dollars, compared to a custom orthotic of $200 or more. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe.
Back ache is easily the most prevalent ailment affecting people today. Around 80 million men and women suffer from back pain at some stage in their life. It is a problem that costs businesses vast amounts of money annually due to time lost and production. New and more effective treatment methods are constantly sought after in the hope of lowering economical impact this issue causes.

Men and women from all corners of the world experience foot ache as a result of leg length discrepancy. In most of these cases Shoe Lifts are usually of very useful. The lifts are capable of decreasing any discomfort and pain in the feet. Shoe Lifts are recommended by countless specialist orthopaedic physicians.
So that they can support the human body in a well-balanced manner, the feet have got a vital function to play. Inspite of that, it can be the most neglected area in the human body. Some people have flat-feet meaning there may be unequal force exerted on the feet. This causes other body parts like knees, ankles and backs to be affected too. Shoe Lifts ensure that proper posture and balance are restored.
Leg length inequality goes largely undiscovered on a daily basis, yet this problem is very easily solved, and can eradicate a number of incidents of back ache.
Treatment for leg length inequality usually involves Shoe Lifts. These are generally cost-effective, usually priced at under twenty dollars, compared to a custom orthotic of $200 or more. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe.
Back ache is easily the most prevalent ailment affecting people today. Around 80 million men and women suffer from back pain at some stage in their life. It is a problem that costs businesses vast amounts of money annually due to time lost and production. New and more effective treatment methods are constantly sought after in the hope of lowering economical impact this issue causes.
Men and women from all corners of the world experience foot ache as a result of leg length discrepancy. In most of these cases Shoe Lifts are usually of very useful. The lifts are capable of decreasing any discomfort and pain in the feet. Shoe Lifts are recommended by countless specialist orthopaedic physicians.
So that they can support the human body in a well-balanced manner, the feet have got a vital function to play. Inspite of that, it can be the most neglected area in the human body. Some people have flat-feet meaning there may be unequal force exerted on the feet. This causes other body parts like knees, ankles and backs to be affected too. Shoe Lifts ensure that proper posture and balance are restored.
What Is A Calcaneal Spur

Overview
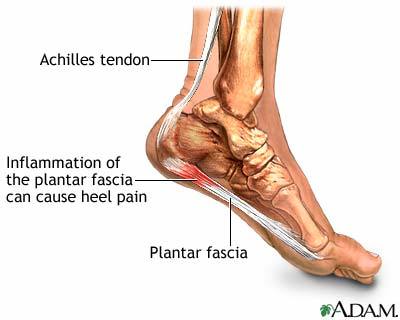
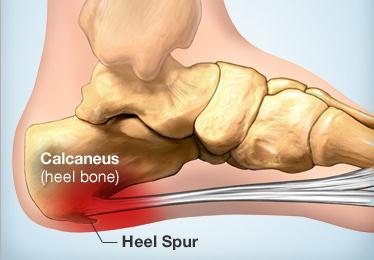
A heel spur is a projection or growth of bone where certain muscles and soft tissue structures of the foot attach to the bottom of the heel. Most commonly, the plantar fascia, a broad, ligament-like structure extending from the heel bone to the base of the toes becomes inflamed, and symptoms of heel pain begin. As this inflammation continues over a period of time, with or without treatment, a heel spur is likely to form. If heel pain is treated early, conservative therapy is often successful, and surgery is usually avoided.
Causes
Common causes of this bone spur in the heel are repetitive trauma to the base of the heel, obesity, poor walking/running technique, poorly fitting shoes, or hereditary conditions.

Symptoms
With heel spurs, people often talk about a dull ache which is felt most of the time with episodes of a sharp pain in the center of the heel or on the inside margin of the heel. Often the pain is worse on first rising in the morning and after rest and is aggravated by prolonged weight bearing and thin-soled shoes.
Diagnosis
Your doctor will review your medical history and examine your foot. X-rays are used to identify the location and size of the heel spur.
Non Surgical Treatment
Rest won?t help you in case of pain from the heel spur. When you get up after sleeping for some time, the pain may get worse. The pain worsens after a period of rest. You will feel pain because the plantar fascia elongates during working which stresses the heel. It is important to see a doctor if you are having consistent pain in you heel. The doctors may advise few or all of the conservative treatments, stretching exercises, shoe recommendations, shoe inserts or orthotic devices, physical therapy, taping or strapping to rest stressed muscles and tendons. There are some over-the-counter medicines available for treatment of heel pain. Acetaminophen (Tylenol), ibuprofen (Advil), or naproxen (Aleve) are some such medicines which can help you to get relief from the pain. In case of biomechanical imbalances causing the pain, a functional orthotic device can help you to get relief. Your doctor may also advise a corticosteroid injection for eliminating the inflammation.
Surgical Treatment
Approximately 2% of people with painful heel spurs need surgery, meaning that 98 out of 100 people do well with the non-surgical treatments previously described. However, these treatments can sometimes be rather long and drawn out, and may become considerably expensive. Surgery should be considered when conservative treatment is unable to control and prevent the pain. If the pain goes away for a while, and continues to come back off and on, despite conservative treatments, surgery should be considered. If the pain really never goes away, but reaches a plateau, beyond which it does not improve despite conservative treatments, surgery should be considered. If the pain requires three or more injections of "cortisone" into the heel within a twelve month period, surgery should be considered.
What Are The Primary Causes Of Posterior Calcaneal Spur

Overview
Patients and doctors often confuse the terms heel spur and plantar fasciitis. While these two diagnoses are related, they are not the same. Plantar fasciitis refers to the inflammation of the plantar fascia--the tissue that forms the arch of the foot. A heel spur is a hook of bone that can form on the heel bone (calcaneus) and is associated with plantar fasciitis. About 70 percent of patients with plantar fasciitis have a heel spur that can be seen on an X-ray. However, many patients without symptoms of pain can have a heel spur. The exact relationship between plantar fasciitis and heel spurs is not entirely understood.
Causes
There exists a membrane that covers most of the bone along the heel. When this membrane gets torn repeatedly due to straining of the muscles in the foot, the calcium deposits that lead to heel spurs are more likely to occur.

Symptoms
The Heel Spur itself is not thought to be painful. Patients who experience pain with Plantar Fasciitis are suffering from inflammation and irritation of the plantar fascia. This the primary cause of pain and not the Heel Spur. Heel Spurs form in some patients who have plantar fasciitis, and tend to occur in patients who have had the problem for a prolonged period of time. While about 70 % of patients with plantar fasciitis have a heel spur, X-rays also show about 50 % of patients with no symptoms of plantar fasciitis also have a heel spur.
Diagnosis
Diagnosis of a heel spur can be done with an x-ray, which will be able to reveal the bony spur. Normally, it occurs where the plantar fascia connects to the heel bone. When the plantar fascia ligament is pulled excessively it begins to pull away from the heel bone. When this excessive pulling occurs, it causes the body to respond by depositing calcium in the injured area, resulting in the formation of the bone spur. The Plantar fascia ligament is a fibrous band of connective tissue running between the heel bone and the ball of the foot. This structure maintains the arch of the foot and distributes weight along the foot as we walk. However, due to the stress that this ligament must endure, it can easily become damaged which commonly occurs along with heel spurs.
Non Surgical Treatment
Common and effective treatments for Heel Spurs include: Stretching exercises, changing to specific shoes, taping or strapping to rest stressed muscles and tendons, custom orthotic devices and physiotherapy. There are many things you can do to treat heel spurs. You should stretch the muscles and ligaments around the area regularly and ensure you are wearing the right footwear for your feet. There are also tapes and straps that you can apply to the muscles and tendons around the area. For more severe cases, custom orthotics may be the way to go along with aggressive physiotherapy. To treat the pain, over the counter NSAIDs (anti-inflammatory medications) is recommended, but use with caution as prolonged use can lead to the development of ulcers. It is therefore best to apply a topical treatment such as Zax?s Original Heelspur Cream, which contains natural ingredients proven to reduce pain and inflammation. More severe forms of the condition may require corticosteroid injections or surgical procedures, but these are very rare cases. Still, should pain become worse and persist, you should consult with your doctor.
Surgical Treatment
In some cases, heel spurs are removed by surgery after an X-ray. While the surgery is typically effective, it?s a timely and expensive procedure. Even after surgery, heel spurs can re-form if the patient continues the lifestyle that led to the problem. These reasons are why most people who develop painful heel spurs begin looking for natural remedies for joint and bone pain. Surgery isn?t required to cure a heel spur. In fact, more than 90 percent of people get better with nonsurgical treatments. If nonsurgical methods fail to treat symptoms of heel spurs after 12 months, surgery may be necessary to alleviate pain and restore mobility.